Publications & Research
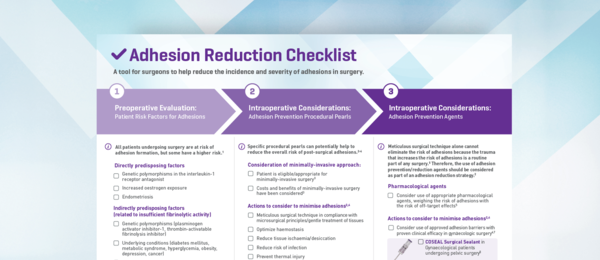
Adhesion Reduction Checklist - GYN
Awareness of consensus recommendations and guidelines for adhesion reduction may reduce the risk of postsurgical adhesions.
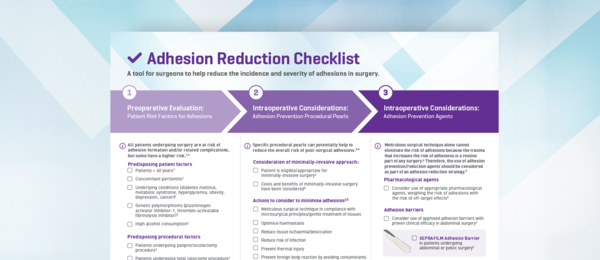
Adhesion Reduction Checklist - CR
Awareness of consensus recommendations and guidelines for adhesion reduction may reduce the risk of postsurgical adhesions.
Adept (icodextrin 4% solution) reduces adhesions after laparoscopic surgery for adhesiolysis: a double-blind, randomized, controlled study
Brown CB, Luciano AA, Martin D, Peers E, Scrimgeour A, diZerega GS; Adept Adhesion Reduction Study Group. Adept (icodextrin 4% solution) reduces adhesions after laparoscopic surgery for adhesiolysis: a double-blind, randomized, controlled study. Fertil Steril. 2007 Nov;88(5):1413-26. doi: 10.1016/j.fertnstert.2006.12.084. Epub 2007 Mar 26. PMID: 17383643.
Prevention of postoperative abdominal adhesions by a sodium hyaluronate-based bioresorbable membrane: a prospective, randomized, double-blind multicenter study
Becker JM, Dayton MT, Fazio VW, Beck DE, Stryker SJ, Wexner SD, Wolff BG, Roberts PL, Smith LE, Sweeney SA, Moore M. Prevention of postoperative abdominal adhesions by a sodium hyaluronate-based bioresorbable membrane: a prospective, randomized, double-blind multicenter study. J Am Coll Surg. 1996 Oct;183(4):297-306. PMID: 8843257.
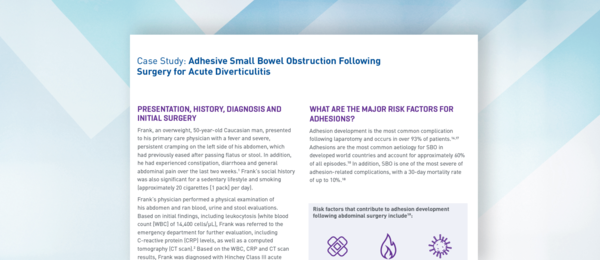
Case Study: Adhesive Small Bowel Obstruction Following Surgery for Acute Diverticulitis
1. Wilkins T, et al. Am Family Phys 2013;87(9):612–620. 2. Sartelli m, et al. World J Emerg Surg 2020;15:32.3.Klarenbeek BR, et al. Int J Colorectal Dis 2012;27:207–214. 4. Chandra V, et al. Arch Surg 2004;139:1221–1224. 5. Halim H, et al. Word J Emerg Surg 2019;14:32. 6. Bridoux V, et al. J Am Coll Surg 2017;225:798-805.
A safety and efficacy study of a resorbable hydrogel for reduction of post-operative adhesions following myomectomy.
Mettler L, Hucke J, Bojar B, Tinneberg H.R, Leyland N, Avelar R. A safety and efficacy study of a resorbable hydrogel for reduction of post-operative adhesions myomectomy. Hum Reprod. 2008 May;23(5):1093-100. doi: 10.1093/humrep/den080. Epub 2008 Mar 17
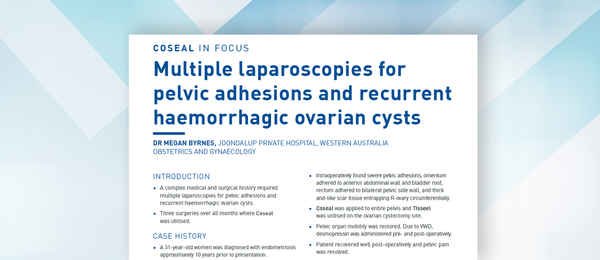
Multiple laparoscopies for pelvic adhesions and recurrent haemorrhagic ovarian cysts.
Case Report: Dr Megan Byrnes B Med Sci, MBBS, FRANZCOG, MRepMed
Joondalup Private Hospital, Western Australia.
Full article housed on learning hub.
Reduction of adhesions after uterine myomectomy by Seprafilm membrane (HAL-F): a blinded, prospective, randomized, multicenter clinical study. Seprafilm Adhesion Study Group
Diamond MP. Reduction of adhesions after uterine myomectomy by Seprafilm membrane (HAL-F): a blinded, prospective, randomized, multicenter clinical study. Seprafilm Adhesion Study Group. Fertil Steril. 1996 Dec;66(6):904-10. PMID: 8941053.

A prospective, randomized, multicenter, controlled study of the safety of Seprafilm adhesion barrier in abdominopelvic surgery of the intestine
Beck DE, Cohen Z, Fleshman JW, Kaufman HS, van Goor H, Wolff BG; Adhesion Study Group Steering Committee. A prospective, randomized, multicenter, controlled study of the safety of Seprafilm adhesion barrier in abdominopelvic surgery of the intestine. Dis Colon Rectum. 2003 Oct;46(10):1310-9. doi: 10.1007/s10350-004-6739-2. PMID: 14530667.

Abdominal adhesions in gynaecologic surgery after caesarean section: a longitudinal population-based register study.
Hesselman S, Hogberg U, Rassjo E-B, Schytt E, Lofgren M, Jonsson M. Abdominal adhesions in gynaecologic surgery after caesarean section: a longitudinal population-based register study. BJOG 2018 Apr;125(5):597-603. doi: 10.1111/1471-0528.14708. Epub 2017 Jun 14
Case Study: Adhesiolysis Following Open Uterine Myomectomy
1 Donnez J, Dolmans MM. Hum Reprod Update 2016;22(6):665–686. 2 Adhesiolysis. E-Book. Published by NCBI (Statpearls). Available at:https://www.ncbi.nlm.nih.gov/ books/NBK563219/ 3 Monk BJ, et al. Am J Obstet Gynecol 1994;170:1396–1403. 4 DeWilde RL, Trew G. Gynecol Surg 2007;4:161–168. 5 Fortin CN, et al. Hum Reprod Update 2015;21(4):536–551.
Intra-abdominal adhesions: definition, origin, significance in surgical practice, and treatment options.
Bruggmann D, Tchartchian G, Wallwiener M, Munstedt K, Tinneberg H-R, Hackethal A.Intra-abdominal adhesions: definition, origin, significance in surgical practice, and treatment options. Dtsch Arztebl Int. 2010 Nov;107(44):769-75. doi: 10.3238/arztebl.2010.0769. Epub 2010 Nov 5
NOTE: This site contains resources which incorporate material contributed or licensed by individuals, companies, or organizations that may be protected by U.S. and foreign copyright laws. These include, but are not limited to PubMed Central (PMC) (see PMC Copyright Notice), Bookshelf (see Bookshelf Copyright Notice), OMIM (see OMIM Copyright Status), and PubChem. All persons reproducing, redistributing, or making commercial use of this information are expected to adhere to the terms and conditions asserted by the copyright holder. Transmission or reproduction of protected items beyond that allowed by fair use (PDF) as defined in the copyright laws requires the written permission of the copyright owners.
Indications and Important Risk Information
FLOSEAL Haemostatic Matrix Indication
FLOSEAL Matrix is indicated in surgical procedures (other than in ophthalmic) as an adjunct to haemostasis when control of bleeding, ranging from oozing to spurting, by ligature or conventional procedures is ineffective or impractical.
Full important risk information
Do not inject or compress FLOSEAL Matrix into blood vessels. Do not apply FLOSEAL Matrix in the absence of active blood flow, e.g., while the vessel is clamped or bypassed, as extensive intravascular clotting and even death may result.
Do not use FLOSEAL Matrix in patients with known allergies to materials of bovine origin. Do not use FLOSEAL Matrix in the closure of skin incisions because it may interfere with the healing of the skin edges.
FLOSEAL Matrix contains Thrombin made from human plasma. It may carry a risk of transmitting infectious agents, e.g., viruses, and theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
FLOSEAL Matrix is not intended as a substitute for meticulous surgical technique and the proper application of ligatures or other conventional procedures for haemostasis.
Excess FLOSEAL Matrix (material not incorporated in the haemostatic clot) should always be removed by gentle irrigation from the site of application.
FLOSEAL Matrix swells by approximately 10% to 20% after product is applied. Maximum swell volume is achieved within about 10 minutes.
The safety and effectiveness of FLOSEAL Matrix has not been established in children under 2 years of age and pregnant women.
Do not use air to remove residual FLOSEAL Matrix from Applicator tip. The Applicator tips should not be cut. Do not use FLOSEAL Matrix on bone surfaces where adhesives, such as methylmethacrylate or other acrylic adhesives, will be required to attach a prosthetic device.
Rx Only. For safe and proper use of this device, refer to the full Instructions for Use.
FLOSEAL Full Instructions for Use:
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
INDICATIONS FOR USE:
Seprafilm is intended as an adjunct in abdominal and pelvic surgery for reducing the incidence, extent and severity of postoperative adhesions at the site of placement, and to reduce adhesive small bowel obstruction when placed in the abdomen.
IMPORTANT RISK INFORMATION
SEPRAFILM Adhesion Barrier is contraindicated in patients with a history of hypersensitivity to Seprafilm and/or to any component of SEPRAFILM. SEPRAFILM Adhesion Barrier is contraindicated for use wrapped directly around a fresh anastomotic suture or staple line; as such use increases the risk of anastomotic leak and related events (fistula, abscess, leak, sepsis, peritonitis). SEPRAFILM Adhesion Barrier must be used according to the instructions for use. SEPRAFILM Adhesion Barrier is for single use only, supplied sterile and must not be re-sterilized. Every opened and unused SEPRAFILM pouch must be discarded. Do not use product if pouch is damaged or opened. The number of sheets used should be just adequate to cover the under surface of the abdominal wall or uterine incision in a single layer.
In patients who have ovarian, primary peritoneal or fallopian tube malignancies, SEPRAFILM use has been reported to have an increased risk of intra-abdominal fluid collection and/or abscess, particularly when extensive debulking surgery was required.
The safety and effectiveness of SEPRAFILM Adhesion Barrier has not been evaluated in clinical studies for the following: Patients with frank infections in the abdominopelvic cavity; patients with abdominopelvic malignancy; device placement in locations other than directly beneath an abdominal wall incision following laparotomy, or directly on the uterus following open myomectomy (not laparoscopic); patients with ongoing local and/or systemic inflammatory cell responses; device use in the presence of other implants, e.g. surgical mesh; patients requiring re-operation within four weeks of SEPRAFILM placement – during anticipated time of peak adhesion formation. Foreign body reactions have occurred with SEPRAFILM Adhesion Barrier.
The safety and effectiveness of SEPRAFILM Adhesion Barrier in combination with other adhesion prevention products and/or in other surgical procedures not within the abdominopelvic cavity have not been established in clinical studies.
The safe and effective use of SEPRAFILM Adhesion Barrier in pregnancy and Cesarean section has not been evaluated. No clinical studies have been conducted in pregnant women or women who have become pregnant within the first month after exposure to SEPRAFILM Adhesion Barrier. Therefore, this product is not recommended for use during pregnancy and avoidance of conception should be considered during the first complete menstrual cycle after use of SEPRAFILM Adhesion Barrier.
Long term clinical outcomes such as chronic pain and infertility have not been determined in clinical studies.
RX Only. For safe and proper use of this device refer to the complete Instructions for Use.
SEPRAFILM Full Instructions For Use
SEPRAFILM Quick Reference Guide
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
ADEPT® Adhesion Reduction Solution [4% Icodextrin] Indications
INDICATIONS ADEPT is indicated to be used in gynaecological laparoscopic surgery of the abdominal-pelvic cavity in adults.
INTENDED USE
ADEPT is intended for use as an intraperitoneal instillate for the reduction of adhesions following gynecological laparoscopic surgery, and should be used as the irrigant during the course of that surgery.
Important Risk Information for ADEPT®
ADEPT® is for direct intraperitoneal administration only. NOT for intravenous (IV) administration.
ADEPT® is contraindicated in patients with known or suspected allergy to cornstarch based polymers e.g. icodextrin, or with
maltose or isomaltose intolerance, or with glycogen storage disease.
ADEPT® is contraindicated in laparotomy, in cases involving bowel resection or repair, or appendectomy and in surgical cases with
frank abdomino-pelvic infection.
There have been rare reports of sterile peritonitis following the use of icodextrin.
Leakage of ADEPT® from port sites may lead to wound healing complications; meticulous fascial closure may reduce leakage
through laparoscopic port sites post-operatively.
There have been rare reports of hypersensitivity reactions, pulmonary edema, pulmonary effusion and arrhythmia.
Anaphylaxis has been reported in a few patients.
Maltose metabolites of icodextrin may interfere with blood glucose measurement in diabetic patients who use rapid blood glucose
systems that are not glucose specific.
In the pivotal study, the most frequently occurring treatment related adverse events between surgeries were post procedural
leaking from port sites, labial, vulvar or vaginal swelling and abdominal distention.
Rx Only: For safe and proper use of this device, please refer to full device Instructions For Use.
Adept Full Instructions for Use
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Coseal Surgical Sealant:
Coseal is indicated for:
Sealing suture lines along arterial and venous reconstructions.
Enforcement of suture and staple lines in lung resection procedures.
Patients under going cardiac surgery to prevent or reduce the incidence, severity and extent of post surgical adhesion formation.
Patients undergoing laparotomic or laparoscopic gynaecological surgery as an adjunct to good surgical technique intended to reduce the incidence, severity and extent of post surgical adhesion formation.
Contraindications:
Do not use COSEAL as a bronchial stump sealant, during bronchial sleeve resections, or for sealing decorticated lung areas. Do not use COSEAL in procedures in which pleural adhesions are desired.
Warnings:
COSEAL swells up to four times its volume within 24 hours of application and additonal swelling occurs as the gel resorbs. Therefore, surgeons should consider the maximum swell volume and its possible effect on surrounding anatomic structures potentially sensitive to compression.
Application involving the use of pressurised gas may be associated with potential risks of air embolism, tissue rupture, or gas entrapment with compression, that may be life-threatening. To minimise these risks control the maximum pressure as indicated in the applicator instructions for use.
Do not inject COSEAL into vessels.
Do not use in place of sutures, staples or mechanical closure.
COSEAL should be used with caution in contaminated areas of the body.
Specifically, do not use COSEAL in contaminated or "dirty" pulmonary resection cases.
Please see the full Instructions for Use for additional information.